Один из .
Но как-то странно, да.
Сами авторы это как аргументируют (помимо абстракта) и есть ли какие-то независимые подтверждения этим аргументам?
Но как-то странно, да.
Сами авторы это как аргументируют (помимо абстракта) и есть ли какие-то независимые подтверждения этим аргументам?
Я странного ничего не вижу. Медицина вообще по некоторым оценкам может регулировать только порядка 10% проблем со здоровьем. Всё остальное - генетика и образ жизни. Комплаентные пациенты (т.е. те, кто соблюдают назначения врача, в том числе и советы по изменению образа жизни) так и так посещают с разумной частотой врачей, а некомплаентным и халява в виде диспансеризации не поможет измениться 
Насчёт независимых подтверждений. Кохрановские обзоры- одна из последних инстанции в таких исследованиях просто по определению. Разве что поискать кохрановские же обзоры по другим странам.
Насчёт независимых подтверждений. Кохрановские обзоры- одна из последних инстанции в таких исследованиях просто по определению. Разве что поискать кохрановские же обзоры по другим странам.
типа запощу текст статьи
Introduction
General health checks have long been common elements of healthcare in some countries such as the United States.1 2 In the UK, the publicly funded NHS Health Check programme was introduced in 2009, and in Denmark an organised health check programme for the general public has been suggested, but now seems abandoned. Health checks are also performed by some primary care physicians outside organised programmes and by commercial clinics.3 However, evidence for their effectiveness has been lacking.
General health checks involve a contact between a person and a healthcare professional to identify signs, symptoms, or risk factors for disease that were previously unrecognised. They are combinations of screening tests, few of which have been adequately studied in randomised trials. For example, although the benefits and harms of treatments for conditions such as hypertension and diabetes have been extensively studied in randomised trials, screening asymptomatic people for these conditions has not.4 5
Health checks are intended to reduce morbidity and prolong life. Theoretically, there are many possible benefits of general health checks, through apparently intuitive mechanisms. The detection of elevated risk factors such as hypertension or hypercholesterolaemia may lead to reductions in morbidity and mortality through preventive treatment. Some tests may detect precursors to disease, such as cervical dysplasia, the treatment of which may prevent cancer from developing. Also, it may be beneficial to detect signs or symptoms of manifest disease that the person had not deemed important. Some people might improve their lifestyle because of the test results and counselling, and healthy people may feel reassured.
While we cannot be certain that general health checks lead to benefit, we know that all medical interventions can lead to harm. Possible harms from health checks are overdiagnosis, overtreatment, distress or injury from invasive follow-up tests, distress due to false positive test results, false reassurance due to false negative test results, possible continuation of adverse health behaviours due to negative test results, adverse psychosocial effects due to labelling, and difficulties with getting insurance. Last but not least, organised programmes of general health checks are likely to be expensive and may result in lost opportunities to improve other areas of healthcare.
Existing reviews on this topic have had narrow definitions of the intervention, included relatively few trials with clinical outcomes, and did not document effects on morbidity or mortality.6 7 8
We aimed to investigate the balance between benefits and harms of general health checks in adult populations, unselected for diseases or risk factors, and performed by any type of healthcare provider. We did not focus on surrogate outcomes because they may be seriously misleading9 and do not capture harmful effects.10 There is also a risk of biased loss to follow-up in non-blinded trials, whereas mortality status can usually be obtained for all randomised people.
Introduction
General health checks have long been common elements of healthcare in some countries such as the United States.1 2 In the UK, the publicly funded NHS Health Check programme was introduced in 2009, and in Denmark an organised health check programme for the general public has been suggested, but now seems abandoned. Health checks are also performed by some primary care physicians outside organised programmes and by commercial clinics.3 However, evidence for their effectiveness has been lacking.
General health checks involve a contact between a person and a healthcare professional to identify signs, symptoms, or risk factors for disease that were previously unrecognised. They are combinations of screening tests, few of which have been adequately studied in randomised trials. For example, although the benefits and harms of treatments for conditions such as hypertension and diabetes have been extensively studied in randomised trials, screening asymptomatic people for these conditions has not.4 5
Health checks are intended to reduce morbidity and prolong life. Theoretically, there are many possible benefits of general health checks, through apparently intuitive mechanisms. The detection of elevated risk factors such as hypertension or hypercholesterolaemia may lead to reductions in morbidity and mortality through preventive treatment. Some tests may detect precursors to disease, such as cervical dysplasia, the treatment of which may prevent cancer from developing. Also, it may be beneficial to detect signs or symptoms of manifest disease that the person had not deemed important. Some people might improve their lifestyle because of the test results and counselling, and healthy people may feel reassured.
While we cannot be certain that general health checks lead to benefit, we know that all medical interventions can lead to harm. Possible harms from health checks are overdiagnosis, overtreatment, distress or injury from invasive follow-up tests, distress due to false positive test results, false reassurance due to false negative test results, possible continuation of adverse health behaviours due to negative test results, adverse psychosocial effects due to labelling, and difficulties with getting insurance. Last but not least, organised programmes of general health checks are likely to be expensive and may result in lost opportunities to improve other areas of healthcare.
Existing reviews on this topic have had narrow definitions of the intervention, included relatively few trials with clinical outcomes, and did not document effects on morbidity or mortality.6 7 8
We aimed to investigate the balance between benefits and harms of general health checks in adult populations, unselected for diseases or risk factors, and performed by any type of healthcare provider. We did not focus on surrogate outcomes because they may be seriously misleading9 and do not capture harmful effects.10 There is also a risk of biased loss to follow-up in non-blinded trials, whereas mortality status can usually be obtained for all randomised people.
Methods
The review was done according to a detailed, peer reviewed protocol, which is available in the Cochrane Library.
Selection criteria
We included randomised trials of general health checks compared with no health checks. The participants had to be 18 years or older and unselected for specific known risk factors or diseases, such as hypertension or heart disease. The setting had to be primary care or the community (that is, we did not include trials in patients recruited from hospital clinics). We accepted trials regardless of the type of provider of the health check and regardless of where the health check was performed (such as general practice or a special clinic).
We defined general health checks as screening for more than one disease or risk factor in more than one organ system, whether performed only once or repeatedly. This definition excludes trials of screening for single diseases in isolation, such as prostate cancer, and trials of single screening tests that may detect more than one disease, such as spirometry. We accepted trials which included a lifestyle intervention (such as advice on diet, smoking, and exercise) in addition to screening, since this is a fairly well defined intervention often incorporated into health checks.
Although we originally planned to include trials of geriatric screening, we found that they included many interventions in addition to screening, such as falls prevention and specialist medication review. Thus, we excluded trials described as specifically targeting older people only, or which only enrolled people aged >65.
Search methods for identification of studies
Studies were identified using the Cochrane Central Register of Controlled Trials (CENTRAL) 2010, issue 11; Medline (via OVID) (1948 to “In-Process”); EMBASE (via OVID) (1947 onwards); Cumulative Index to Nursing and Allied Health Literature (CINAHL); EbscoHost (1980 onwards); Healthstar (via OVID) (1966 to 2010); and the EPOC Specialised Register. Related systematic reviews were identified by searching the Database of Abstracts of Reviews of Effectiveness (DARE and ongoing trials were identified by searching ClinicalTrials.gov and WHO ICTRP. The searches were conducted in November and December 2010 and updated in July 2012. An example of a search strategy is available in appendix 1 on bmj.com.
Two observers searched the reference lists of included articles, and one author used citation tracking (Web of Knowledge) on all articles describing eligible trials. We asked authors of the included studies if they were aware of any other published, unpublished, or ongoing studies that could meet our inclusion criteria.
Selection of studies
Two observers (LTK and CGL or KJJ) independently assessed the potential relevance of all titles and abstracts identified through the searches. Full text copies of potentially relevant articles were assessed for eligibility independently by two authors (LTK and CGL or KJJ). Disagreements were resolved through discussion, involving the other authors (KJJ and PCG) when necessary.
Two authors (LTK and KJJ) independently extracted pre-specified data items from the included articles in a non-blinded fashion and entered them into a pilot tested data extraction form. When our preferred data formats were not available, we extracted what was possible, including narrative accounts if numbers were missing. We preferentially extracted data allowing an intention to treat analysis. We attempted to contact authors when necessary and succeeded in 10 cases.
Two authors (LTK and KJJ) independently assessed risk of bias in the included trials using the Cochrane Risk of Bias tool. The domains formally assessed were sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Baseline balance and risk of contamination was also assessed.
Analysis
Our primary outcomes were total mortality and disease-specific mortality. Our secondary outcomes were morbidity (such as myocardial infarction number of new diagnoses (total and condition-specific admission to hospital, disability, patient worry, self reported health, number of referrals to specialists, number of non-scheduled visits to general practitioners, number of additional diagnostic procedures due to positive screening tests, new medications prescribed, frequency and type of surgery, and absence from work.
When cardiovascular and cancer mortality were reported as such, we used those numbers. When they were reported in several disease categories or organ systems, two of us independently combined them into an overall measure of cardiovascular or cancer mortality. For example, in one trial we added fatal coronary heart disease and fatal stroke to give a measure of cardiovascular mortality.
Meta-analysis was feasible only for our primary outcomes. We calculated risk ratios with 95% confidence intervals using the random effects model. To allow incorporation of adjusted effect estimates we used the generic inverse variance approach. Heterogeneity was investigated with the I2 statistic.
We conducted the following pre-specified subgroup analyses: one versus multiple health checks, lifestyle intervention versus no lifestyle intervention, length of follow-up (≤5 years versus >5 years trial age (started before 1980 versus after 1980 geographical location (Europe versus US examination by a physician, and risk of bias (selection bias, performance bias, detection bias, attrition bias, contamination). We did one pre-specified sensitivity analysis, excluding cluster randomised trials, and one post hoc sensitivity analysis excluding trials judged to be biased towards no effect. The results of these are presented in the corresponding Cochrane review.11 For other outcomes, we summarised the results in tables and did a qualitative synthesis.
The review was done according to a detailed, peer reviewed protocol, which is available in the Cochrane Library.
Selection criteria
We included randomised trials of general health checks compared with no health checks. The participants had to be 18 years or older and unselected for specific known risk factors or diseases, such as hypertension or heart disease. The setting had to be primary care or the community (that is, we did not include trials in patients recruited from hospital clinics). We accepted trials regardless of the type of provider of the health check and regardless of where the health check was performed (such as general practice or a special clinic).
We defined general health checks as screening for more than one disease or risk factor in more than one organ system, whether performed only once or repeatedly. This definition excludes trials of screening for single diseases in isolation, such as prostate cancer, and trials of single screening tests that may detect more than one disease, such as spirometry. We accepted trials which included a lifestyle intervention (such as advice on diet, smoking, and exercise) in addition to screening, since this is a fairly well defined intervention often incorporated into health checks.
Although we originally planned to include trials of geriatric screening, we found that they included many interventions in addition to screening, such as falls prevention and specialist medication review. Thus, we excluded trials described as specifically targeting older people only, or which only enrolled people aged >65.
Search methods for identification of studies
Studies were identified using the Cochrane Central Register of Controlled Trials (CENTRAL) 2010, issue 11; Medline (via OVID) (1948 to “In-Process”); EMBASE (via OVID) (1947 onwards); Cumulative Index to Nursing and Allied Health Literature (CINAHL); EbscoHost (1980 onwards); Healthstar (via OVID) (1966 to 2010); and the EPOC Specialised Register. Related systematic reviews were identified by searching the Database of Abstracts of Reviews of Effectiveness (DARE and ongoing trials were identified by searching ClinicalTrials.gov and WHO ICTRP. The searches were conducted in November and December 2010 and updated in July 2012. An example of a search strategy is available in appendix 1 on bmj.com.
Two observers searched the reference lists of included articles, and one author used citation tracking (Web of Knowledge) on all articles describing eligible trials. We asked authors of the included studies if they were aware of any other published, unpublished, or ongoing studies that could meet our inclusion criteria.
Selection of studies
Two observers (LTK and CGL or KJJ) independently assessed the potential relevance of all titles and abstracts identified through the searches. Full text copies of potentially relevant articles were assessed for eligibility independently by two authors (LTK and CGL or KJJ). Disagreements were resolved through discussion, involving the other authors (KJJ and PCG) when necessary.
Two authors (LTK and KJJ) independently extracted pre-specified data items from the included articles in a non-blinded fashion and entered them into a pilot tested data extraction form. When our preferred data formats were not available, we extracted what was possible, including narrative accounts if numbers were missing. We preferentially extracted data allowing an intention to treat analysis. We attempted to contact authors when necessary and succeeded in 10 cases.
Two authors (LTK and KJJ) independently assessed risk of bias in the included trials using the Cochrane Risk of Bias tool. The domains formally assessed were sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Baseline balance and risk of contamination was also assessed.
Analysis
Our primary outcomes were total mortality and disease-specific mortality. Our secondary outcomes were morbidity (such as myocardial infarction number of new diagnoses (total and condition-specific admission to hospital, disability, patient worry, self reported health, number of referrals to specialists, number of non-scheduled visits to general practitioners, number of additional diagnostic procedures due to positive screening tests, new medications prescribed, frequency and type of surgery, and absence from work.
When cardiovascular and cancer mortality were reported as such, we used those numbers. When they were reported in several disease categories or organ systems, two of us independently combined them into an overall measure of cardiovascular or cancer mortality. For example, in one trial we added fatal coronary heart disease and fatal stroke to give a measure of cardiovascular mortality.
Meta-analysis was feasible only for our primary outcomes. We calculated risk ratios with 95% confidence intervals using the random effects model. To allow incorporation of adjusted effect estimates we used the generic inverse variance approach. Heterogeneity was investigated with the I2 statistic.
We conducted the following pre-specified subgroup analyses: one versus multiple health checks, lifestyle intervention versus no lifestyle intervention, length of follow-up (≤5 years versus >5 years trial age (started before 1980 versus after 1980 geographical location (Europe versus US examination by a physician, and risk of bias (selection bias, performance bias, detection bias, attrition bias, contamination). We did one pre-specified sensitivity analysis, excluding cluster randomised trials, and one post hoc sensitivity analysis excluding trials judged to be biased towards no effect. The results of these are presented in the corresponding Cochrane review.11 For other outcomes, we summarised the results in tables and did a qualitative synthesis.
Results
Results of the search
We identified 16 eligible trials, but two of these never published results.12 13 Thus, we analysed 14 trials, of which nine had data on mortality (fig 1⇓).
Study characteristics
The 14 trials analysed included a total of 182 880 participants, with 76 403 allocated to health checks and 106 477 to control groups. The length of follow-up varied from 1 to 22 years (table 1⇓). The participants were recruited from general practice in five trials,14 15 16 17 18 the general population in seven trials,19 20 21 22 23 24 25 health plan members in one trial,26 and the workplace in one trial.27 The health checks took place in general practice in four trials, a screening clinic in five trials, at the workplace in one trial, in a hospital in one trial, and in three trials it was not clear. Table 2⇓ provides a summary of the trials’ methods, and table 3⇓ provides an overview of the screening tests used.
Risk of bias in included studies
Risk of bias varied between trials, and within trials for different outcomes (fig 2⇓). Most trials randomised participants before any contact was made, effectively leading to concealed allocation. When the randomisation sequence was predictable but likely to provide balanced groups given allocation before contact (such as date of birth we judged the risk of selection bias to be low.15 19 20 26 Of the nine trials that reported mortality,14 16 18 19 20 21 22 26 27 seven had a low risk of selection bias, and eight had a low risk of attrition bias for that particular outcome. All nine trials reporting mortality could be analysed by intention to treat. By design, three trials were biased towards no effect.14 18 26 In two of these, the control group was offered health checks before follow-up for mortality ended. In one, the control group had free access to the same health check as the intervention group and, though not actively encouraged, used this option to a considerable extent. In four trials, the follow-up and treatment of detected abnormalities were possibly better in the intervention group than in the control group (for example, follow-up by specialists who used treatment algorithms).19 20 22 27 This might have caused bias in favour of screening.
For our secondary outcomes, lack of blinding and missing outcome data were major issues. Funnel plots did not show asymmetry, but the number of trials is low (figs 3-5⇓ ⇓ ⇓).
Effects of interventions
Total mortality
Nine trials reported on total mortality, and our meta-analysis included 155 899 people and 11 940 deaths. The median length of follow-up was nine years (range 4–22 years and the median event rate in the control groups was 7% (range 2%–16%). We did not find an effect of general health checks on total mortality, risk ratio 0.99 (95% confidence interval 0.95 to 1.03) (fig 6⇓). There was no heterogeneity (I2=0%). Subgroup and sensitivity analyses did not alter this result.
Cause-specific mortality
For cardiovascular mortality (8 trials, 152 435 people, 4567 deaths the median length of follow-up was 10.4 years and the median event rate in the control groups was 3.7%. The pooled estimate was risk ratio 1.03 (0.91 to 1.17 but with large heterogeneity (I2=64%) (fig 7⇓). Subgroup and sensitivity analyses did not alter the results, nor explain the heterogeneity. One possible explanation for the heterogeneity is the varying definitions of the outcome among trials. One trial found a large beneficial effect,20 and one found a large harmful effect.14
For cancer mortality (8 trials, 139 290people, 3663 deaths the median length of follow-up was 10.4 years, and the median event rate in the control groups was 2.4%. The pooled estimate was risk ratio 1.01 (0.92 to 1.12) with moderate heterogeneity (I2=33%) (fig 8⇓). A high quality trial found a reduction in cancer mortality (risk ratio 0.87 (0.76 to 0.99.22 That trial did not use cancer screening tests, and was not successful in reducing smoking.
Subgroup and sensitivity analyses
The pre-specified subgroup analyses resulted in groups with few trials, and the results should be viewed with caution. We did not find any convincing patterns or explanations for the heterogeneity observed.
For cancer mortality, three trials that used only one health check showed a trend towards harm (relative risk 1.10 (1.00 to 1.21 and five trials that used more than one health check showed a trend towards benefit (relative risk 0.92 (0.83 to 1.02. The test for subgroup differences was significant (P = 0.01).
For cardiovascular mortality, the reverse pattern was present. The three trials using only one health check showed a trend towards benefit (relative risk 0.89 (0.69 to 1.14 and the five trials using more than one health check showed a trend towards harm (relative risk 1.11 (0.95 to 1.30. The test for subgroup differences was not significant (P=0.13).
In a post hoc sensitivity analysis, we removed the three trials that were biased towards no effect14 18 26 and one trial in which we had prioritised power over contrast in the merging of three intervention groups.16 This did not change the results for total mortality (relative risk 0.98 (0.94 to 1.02 cardiovascular mortality (0.97 (0.86 to 1.09 or cancer mortality (1.01 (0.88 to 1.17.
Secondary outcomes
We refer the reader to appendix 2 on bmj.com for detailed results for our secondary outcomes. In summary, we did not find an effect on clinical events, such as coronary heart disease, or other measures of morbidity, but they were infrequently reported. One trial found an increased occurrence of hypertension and hypercholesterolaemia with screening. One trial found a 20% increase in the total number of new diagnoses per participant over six years compared with the control group and an increased occurrence of self reported chronic disease. Other trials reported large numbers of abnormalities detected at the health checks. No trials compared the total number of prescriptions, but two out of four trials found an increased number of people using antihypertensive drugs. Two out of four trials found small beneficial effects on self reported health, but this could be due to reporting bias as the trials were not blinded. We did not find an effect on admission to hospital, disability, worry, additional visits to the physician, or absence from work, but most of these outcomes were poorly studied. We did not find useful results on the number of referrals to specialists, the number of follow-up tests after positive screening results, or the amount of surgery used.
Results of the search
We identified 16 eligible trials, but two of these never published results.12 13 Thus, we analysed 14 trials, of which nine had data on mortality (fig 1⇓).
Study characteristics
The 14 trials analysed included a total of 182 880 participants, with 76 403 allocated to health checks and 106 477 to control groups. The length of follow-up varied from 1 to 22 years (table 1⇓). The participants were recruited from general practice in five trials,14 15 16 17 18 the general population in seven trials,19 20 21 22 23 24 25 health plan members in one trial,26 and the workplace in one trial.27 The health checks took place in general practice in four trials, a screening clinic in five trials, at the workplace in one trial, in a hospital in one trial, and in three trials it was not clear. Table 2⇓ provides a summary of the trials’ methods, and table 3⇓ provides an overview of the screening tests used.
Risk of bias in included studies
Risk of bias varied between trials, and within trials for different outcomes (fig 2⇓). Most trials randomised participants before any contact was made, effectively leading to concealed allocation. When the randomisation sequence was predictable but likely to provide balanced groups given allocation before contact (such as date of birth we judged the risk of selection bias to be low.15 19 20 26 Of the nine trials that reported mortality,14 16 18 19 20 21 22 26 27 seven had a low risk of selection bias, and eight had a low risk of attrition bias for that particular outcome. All nine trials reporting mortality could be analysed by intention to treat. By design, three trials were biased towards no effect.14 18 26 In two of these, the control group was offered health checks before follow-up for mortality ended. In one, the control group had free access to the same health check as the intervention group and, though not actively encouraged, used this option to a considerable extent. In four trials, the follow-up and treatment of detected abnormalities were possibly better in the intervention group than in the control group (for example, follow-up by specialists who used treatment algorithms).19 20 22 27 This might have caused bias in favour of screening.
For our secondary outcomes, lack of blinding and missing outcome data were major issues. Funnel plots did not show asymmetry, but the number of trials is low (figs 3-5⇓ ⇓ ⇓).
Effects of interventions
Total mortality
Nine trials reported on total mortality, and our meta-analysis included 155 899 people and 11 940 deaths. The median length of follow-up was nine years (range 4–22 years and the median event rate in the control groups was 7% (range 2%–16%). We did not find an effect of general health checks on total mortality, risk ratio 0.99 (95% confidence interval 0.95 to 1.03) (fig 6⇓). There was no heterogeneity (I2=0%). Subgroup and sensitivity analyses did not alter this result.
Cause-specific mortality
For cardiovascular mortality (8 trials, 152 435 people, 4567 deaths the median length of follow-up was 10.4 years and the median event rate in the control groups was 3.7%. The pooled estimate was risk ratio 1.03 (0.91 to 1.17 but with large heterogeneity (I2=64%) (fig 7⇓). Subgroup and sensitivity analyses did not alter the results, nor explain the heterogeneity. One possible explanation for the heterogeneity is the varying definitions of the outcome among trials. One trial found a large beneficial effect,20 and one found a large harmful effect.14
For cancer mortality (8 trials, 139 290people, 3663 deaths the median length of follow-up was 10.4 years, and the median event rate in the control groups was 2.4%. The pooled estimate was risk ratio 1.01 (0.92 to 1.12) with moderate heterogeneity (I2=33%) (fig 8⇓). A high quality trial found a reduction in cancer mortality (risk ratio 0.87 (0.76 to 0.99.22 That trial did not use cancer screening tests, and was not successful in reducing smoking.
Subgroup and sensitivity analyses
The pre-specified subgroup analyses resulted in groups with few trials, and the results should be viewed with caution. We did not find any convincing patterns or explanations for the heterogeneity observed.
For cancer mortality, three trials that used only one health check showed a trend towards harm (relative risk 1.10 (1.00 to 1.21 and five trials that used more than one health check showed a trend towards benefit (relative risk 0.92 (0.83 to 1.02. The test for subgroup differences was significant (P = 0.01).
For cardiovascular mortality, the reverse pattern was present. The three trials using only one health check showed a trend towards benefit (relative risk 0.89 (0.69 to 1.14 and the five trials using more than one health check showed a trend towards harm (relative risk 1.11 (0.95 to 1.30. The test for subgroup differences was not significant (P=0.13).
In a post hoc sensitivity analysis, we removed the three trials that were biased towards no effect14 18 26 and one trial in which we had prioritised power over contrast in the merging of three intervention groups.16 This did not change the results for total mortality (relative risk 0.98 (0.94 to 1.02 cardiovascular mortality (0.97 (0.86 to 1.09 or cancer mortality (1.01 (0.88 to 1.17.
Secondary outcomes
We refer the reader to appendix 2 on bmj.com for detailed results for our secondary outcomes. In summary, we did not find an effect on clinical events, such as coronary heart disease, or other measures of morbidity, but they were infrequently reported. One trial found an increased occurrence of hypertension and hypercholesterolaemia with screening. One trial found a 20% increase in the total number of new diagnoses per participant over six years compared with the control group and an increased occurrence of self reported chronic disease. Other trials reported large numbers of abnormalities detected at the health checks. No trials compared the total number of prescriptions, but two out of four trials found an increased number of people using antihypertensive drugs. Two out of four trials found small beneficial effects on self reported health, but this could be due to reporting bias as the trials were not blinded. We did not find an effect on admission to hospital, disability, worry, additional visits to the physician, or absence from work, but most of these outcomes were poorly studied. We did not find useful results on the number of referrals to specialists, the number of follow-up tests after positive screening results, or the amount of surgery used.
Discussion
Summary of main results
We did not find an effect on total or cause-specific mortality from general health checks in adult populations unselected for risk factors or disease. For total mortality, our confidence interval includes a 5% reduction and a 3% increase, both of which would be clinically relevant. However, for the causes of death most likely to be influenced by health checks, cardiovascular mortality and cancer mortality, there were no reductions either. A substantial latency of effects on mortality would be expected, but we included several trials with very long follow-up, and they did not show a benefit. Neither did we find a difference in effects in our subgroup analysis comparing trials with up to five years of follow-up with trials with more than five years of follow-up. The results suggest that the lack of effect on total mortality is not a chance finding or due to low power, but that there is no, or only a minimal, effect of the intervention on mortality in general adult populations. We did not include geriatric trials, and our results therefore do not apply to this population.
We also looked at several other outcomes that might be influenced by health checks, but most of these were either infrequently reported or the results were at high risk of bias because of the inevitable lack of blinding and consequent risk of reporting bias and biased loss to follow-up. We did find that health checks led to more diagnoses and more medical treatment for hypertension, as expected, but, as these did not improve mortality or morbidity, they may be considered harms rather than benefits. Two trials found improved self reported health, but the effects were small and could be due to bias.
Strengths and weaknesses of the review
The main strength of this review is our attempt to reduce bias in the review process by conducting it according to a published and peer reviewed Cochrane protocol and by following empirically founded review guidelines. We identified more relevant trials than previous reviews and did a thorough data collection and appraisal of included studies.
The main limitations are the risk of bias in some of the included trials, their age, and infrequent and poor reporting of some of our specified outcomes, in particular the harms. Another possible limitation is the clinical and methodological heterogeneity among the included trials, although the results were generally consistent for the frequently reported outcomes.
Strengths and weaknesses in relation to other studies
A systematic review of “the periodic health evaluation” included both trials and observational studies, and also geriatric studies, but it used a different definition of the intervention.6 The trials reviewed by us are mostly different ones, but the results are broadly similar with regard to the outcomes that were assessed in both reviews: total mortality, hospitalisation, disability, and the number of new diagnoses (disease detection). In terms of the effects of health checks on participants’ health worries, the previous review found one geriatric trial with a beneficial effect, whereas we found two trials with no effect on this outcome. Other reviews studied the effect of calculating and communicating coronary risk, but had a more narrow definition of the intervention, and did not find results on morbidity and mortality.7 8
In order to get the most reliable answers to our questions, we did not include observational studies because the influence of self selection bias is too great compared with the expected small effect of an intervention in a predominantly healthy population. We also chose not to focus on surrogate outcomes such as changes in risk factors or delivery of preventive services, as these may be misleading because an improvement does not necessarily benefit the participant and because they do not measure harms. Nevertheless, we succeeded in identifying several trials that addressed our research questions.
We did not include geriatric trials because they included additional interventions likely to affect the outcomes. A systematic review found that geriatric assessments for general elderly populations reduced the risk of not living at home and of being admitted to a nursing home, but did not find an effect on mortality.28
Meaning of the study
The lack of beneficial effects indicates that the interventions did not work as intended in the included trials. There are several possible explanations for this. Most of the trials were old and consequently used treatments different from what would be used today—such as clofibrate or nicotinic acid for hypercholesterolaemia, instead of statins. Also, thresholds for treating cardiovascular risk factors were higher than they are today. However, it is not a given that the results would be better today, as medical innovations sometimes prove harmful29 and as reducing risk factor thresholds means treating people at lower risk who have a smaller potential for benefit but the same risk of harm.30 Another possibility is that preventive drugs could have a less favourable balance between benefits and harms when used in general populations compared with in pharmacological trials, which often use many exclusion criteria.31 In our meta-analyses, arranged by year of trial start, there are no visible time trends and the idea of increasing benefits over time remains hypothetical. The results on mortality from the Inter99 trial 25 will be published soon and will inform about the effect of health checks in a modern setting.
Finally, some of the trials used only one health check instead of repeated health checks. For cancer mortality, subgroup analysis showed a trend towards benefit from more than one health check and towards harm from one health check only. For cardiovascular mortality, the opposite trends were observed. We regard these results as chance findings. Also, it is not a given that several health checks would be better than one, as some of the harms would increase.
Two other factors are probably important for explaining our results. First, people who accept an invitation to a health check are often different from those who do not. They tend to have higher socioeconomic status,32 lower cardiovascular risk,33 less cardiovascular morbidity,25 and lower mortality.22 Thus, systematic health checks may not reach those who need prevention the most, and they have been described as another example of inverse care.33 Second, many physicians already carry out testing for cardiovascular risk factors or diseases in patients whom they judge to be at risk when they see them for other reasons. This is often considered an integral part of primary care. Such clinically motivated testing may already have identified many people with disease or elevated risk factors, thus eroding the potential for a benefit from systematic screening.
Our results do not support the use of general health checks aimed at a general adult population outside the context of randomised trials. However, they do not imply that physicians should stop clinically motivated testing and preventive activities, as these may be an important reason why systematic health checks showed no effect. Also, our results do not imply that all individual components of the health checks are ineffective, since effects of harmful components may have balanced out effects of beneficial ones.
Future research
We suggest that future research is directed at the individual components of health checks, such as screening for cardiovascular risk factors, chronic obstructive pulmonary disease, diabetes, or kidney disease. We also suggest that surrogate outcomes such as changes in risk factors are not used for assessing the benefits of health checks. The large randomised trials with long follow-up that are required are expensive, but not nearly as expensive as the implementation of ineffective or harmful general health check programmes.
Summary of main results
We did not find an effect on total or cause-specific mortality from general health checks in adult populations unselected for risk factors or disease. For total mortality, our confidence interval includes a 5% reduction and a 3% increase, both of which would be clinically relevant. However, for the causes of death most likely to be influenced by health checks, cardiovascular mortality and cancer mortality, there were no reductions either. A substantial latency of effects on mortality would be expected, but we included several trials with very long follow-up, and they did not show a benefit. Neither did we find a difference in effects in our subgroup analysis comparing trials with up to five years of follow-up with trials with more than five years of follow-up. The results suggest that the lack of effect on total mortality is not a chance finding or due to low power, but that there is no, or only a minimal, effect of the intervention on mortality in general adult populations. We did not include geriatric trials, and our results therefore do not apply to this population.
We also looked at several other outcomes that might be influenced by health checks, but most of these were either infrequently reported or the results were at high risk of bias because of the inevitable lack of blinding and consequent risk of reporting bias and biased loss to follow-up. We did find that health checks led to more diagnoses and more medical treatment for hypertension, as expected, but, as these did not improve mortality or morbidity, they may be considered harms rather than benefits. Two trials found improved self reported health, but the effects were small and could be due to bias.
Strengths and weaknesses of the review
The main strength of this review is our attempt to reduce bias in the review process by conducting it according to a published and peer reviewed Cochrane protocol and by following empirically founded review guidelines. We identified more relevant trials than previous reviews and did a thorough data collection and appraisal of included studies.
The main limitations are the risk of bias in some of the included trials, their age, and infrequent and poor reporting of some of our specified outcomes, in particular the harms. Another possible limitation is the clinical and methodological heterogeneity among the included trials, although the results were generally consistent for the frequently reported outcomes.
Strengths and weaknesses in relation to other studies
A systematic review of “the periodic health evaluation” included both trials and observational studies, and also geriatric studies, but it used a different definition of the intervention.6 The trials reviewed by us are mostly different ones, but the results are broadly similar with regard to the outcomes that were assessed in both reviews: total mortality, hospitalisation, disability, and the number of new diagnoses (disease detection). In terms of the effects of health checks on participants’ health worries, the previous review found one geriatric trial with a beneficial effect, whereas we found two trials with no effect on this outcome. Other reviews studied the effect of calculating and communicating coronary risk, but had a more narrow definition of the intervention, and did not find results on morbidity and mortality.7 8
In order to get the most reliable answers to our questions, we did not include observational studies because the influence of self selection bias is too great compared with the expected small effect of an intervention in a predominantly healthy population. We also chose not to focus on surrogate outcomes such as changes in risk factors or delivery of preventive services, as these may be misleading because an improvement does not necessarily benefit the participant and because they do not measure harms. Nevertheless, we succeeded in identifying several trials that addressed our research questions.
We did not include geriatric trials because they included additional interventions likely to affect the outcomes. A systematic review found that geriatric assessments for general elderly populations reduced the risk of not living at home and of being admitted to a nursing home, but did not find an effect on mortality.28
Meaning of the study
The lack of beneficial effects indicates that the interventions did not work as intended in the included trials. There are several possible explanations for this. Most of the trials were old and consequently used treatments different from what would be used today—such as clofibrate or nicotinic acid for hypercholesterolaemia, instead of statins. Also, thresholds for treating cardiovascular risk factors were higher than they are today. However, it is not a given that the results would be better today, as medical innovations sometimes prove harmful29 and as reducing risk factor thresholds means treating people at lower risk who have a smaller potential for benefit but the same risk of harm.30 Another possibility is that preventive drugs could have a less favourable balance between benefits and harms when used in general populations compared with in pharmacological trials, which often use many exclusion criteria.31 In our meta-analyses, arranged by year of trial start, there are no visible time trends and the idea of increasing benefits over time remains hypothetical. The results on mortality from the Inter99 trial 25 will be published soon and will inform about the effect of health checks in a modern setting.
Finally, some of the trials used only one health check instead of repeated health checks. For cancer mortality, subgroup analysis showed a trend towards benefit from more than one health check and towards harm from one health check only. For cardiovascular mortality, the opposite trends were observed. We regard these results as chance findings. Also, it is not a given that several health checks would be better than one, as some of the harms would increase.
Two other factors are probably important for explaining our results. First, people who accept an invitation to a health check are often different from those who do not. They tend to have higher socioeconomic status,32 lower cardiovascular risk,33 less cardiovascular morbidity,25 and lower mortality.22 Thus, systematic health checks may not reach those who need prevention the most, and they have been described as another example of inverse care.33 Second, many physicians already carry out testing for cardiovascular risk factors or diseases in patients whom they judge to be at risk when they see them for other reasons. This is often considered an integral part of primary care. Such clinically motivated testing may already have identified many people with disease or elevated risk factors, thus eroding the potential for a benefit from systematic screening.
Our results do not support the use of general health checks aimed at a general adult population outside the context of randomised trials. However, they do not imply that physicians should stop clinically motivated testing and preventive activities, as these may be an important reason why systematic health checks showed no effect. Also, our results do not imply that all individual components of the health checks are ineffective, since effects of harmful components may have balanced out effects of beneficial ones.
Future research
We suggest that future research is directed at the individual components of health checks, such as screening for cardiovascular risk factors, chronic obstructive pulmonary disease, diabetes, or kidney disease. We also suggest that surrogate outcomes such as changes in risk factors are not used for assessing the benefits of health checks. The large randomised trials with long follow-up that are required are expensive, but not nearly as expensive as the implementation of ineffective or harmful general health check programmes.
картинки типа таких
Fig 8 Forest plot showing effect of general health checks on cancer mortality. Year indicates the year of trial start
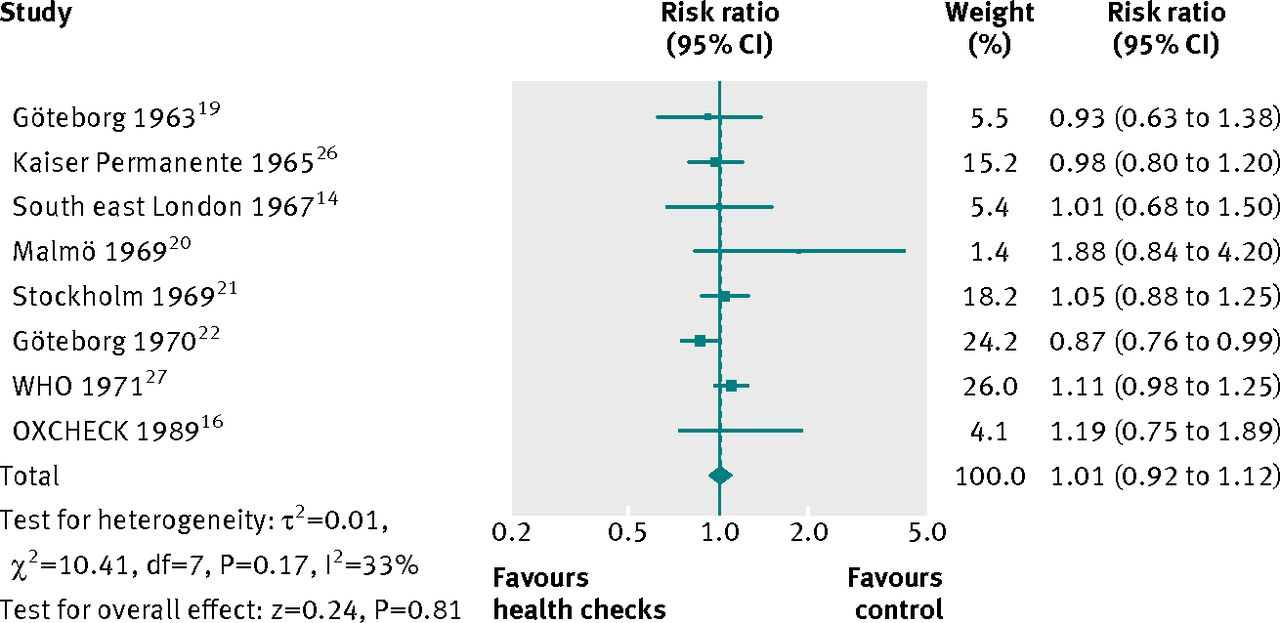
Fig 8 Forest plot showing effect of general health checks on cancer mortality. Year indicates the year of trial start
No benefit from general health checksПускай они себе свое мнение в жопу засунут.
Проще заранее обследовать группы риска и профилактировать их, чем потом лечить.
К тому же надо учитывать, когда и в каких условиях это все создавалось. В 50-е, 60-е и позже было не очень много возможностей у медицины и профилактика на ранних стадиях сильно повышала шанс выздоровления при онкологии, например.
Пускай они себе свое мнение в жопу засунут.Пофи, бери методику, результаты и критикуй, предметно и обоснованно критикуй. Если что, это и есть доказательная медицина-когда не предполагать надо на основе умозрительных рассуждений, а брать и доказывать с циферками в руках.
Про комплаентность ты пропустил просто в принципе мимо ушей. Про рак - да не обнаруживается он массово на диспансеризациях на такой стадии и в такой пропорции стадий, которая бы снизила в итоге смертность от рака. Если у пациента нет мозгов, чтобы определиться с индивидуальными рисками прицельно, а потом регулировать посещения именно так, чтоб почаще уточнять показатели в области личных рисков, и пореже - остальные, то никакие диспансеризации ничего ему особо не обнаружат. Что, раковая настороженность откуда-то возьмётся у всей врачебной братии? Или КТ\ МРТ\ Колоноскопия и т.д. в районной поликлинике нарисуются в день фиксации неспецических жалоб , которые подходят к куче диагнозов, и рак на 1 стадии там будет далеко не в лидерах. Полезны прицельные скриннинги - так это и сами авторы пишут. Но диспансеризации как таковые - это деньги, выброшенные на ветер.
А вообще при вопросе о диспансеризациях мне всегда вспоминаются осмотры детей,во время которых асимметрия позвоночника обнаруживалась редкой, а потом раз - и сколиоз в школе
 В развитиых странах обнаруживалась у всех с будущим сколиозом без травматического сколиоза, а в СССР - неа. Страна уникумов, ёпта
В развитиых странах обнаруживалась у всех с будущим сколиозом без травматического сколиоза, а в СССР - неа. Страна уникумов, ёптапрофилактика на ранних стадиях сильно повышала шанс выздоровления при онкологии, напримерА можно поподробнее про профилактику на ранних стадиях и выздоровление при онкологии?

про онкологию же картинка как раз
А пока ему на русском в афтершок убедительно не рассказали, что буржуи лохи и глупцы, он не способен предметно говорить совсем. Так только, косноязычно про связь диспансеризации и профилактику рака на ранней стадии выдать может. Не поступили ещё чётко, ясно и подробно написанные инструкции
Самое интересное, что как минимум профилактика колоректального рака без наследственного полипоза кишечника и всяких синдромов действительно есть. Только понятно, что не на ранней стадии -там уже о профилактике говорить поздно в принципе. Только диспансеризация для этого нафиг не нужна - достаточно посетить нормального терапевта или онколога хотя бы раз в жизни и поинтересоваться этим.
Самое интересное, что как минимум профилактика колоректального рака без наследственного полипоза кишечника и всяких синдромов действительно есть. Только понятно, что не на ранней стадии -там уже о профилактике говорить поздно в принципе. Только диспансеризация для этого нафиг не нужна - достаточно посетить нормального терапевта или онколога хотя бы раз в жизни и поинтересоваться этим.
ти сомневаешься в наличии пользы от диспансеризации или что ты еще хотела сказать?
судя по картинке выше, она нулевая
нед
и я поясню почему
вы берете сугубо медицинский аспект, но как-то забываете, что люди существа ленивые и даже ради заботы о здоровье не будут регулярно куда-то ходить
особенно если ради этого надо предпринимать дополнительные усилия
даже сейчас многие не хрдят регулярно к стоматологу, а только когда заболит
и я поясню почему
вы берете сугубо медицинский аспект, но как-то забываете, что люди существа ленивые и даже ради заботы о здоровье не будут регулярно куда-то ходить
особенно если ради этого надо предпринимать дополнительные усилия
даже сейчас многие не хрдят регулярно к стоматологу, а только когда заболит
можешь почитать как в проебалтике врач плачется о совковых временах
http://ursa-tm.ru/forum/index.php?/topic/55100-%E0%EA%E0%E4%...
http://ursa-tm.ru/forum/index.php?/topic/55100-%E0%EA%E0%E4%...
Опиши, как терапевт на диспансеризации должен обнаруживать рак почти любого внутреннего органа на 1 операбельной стадии без КТ\ МРТ\ колоноскопии, которые требовалось бы с этой целью назначить поголовно всем пришедшим на диспансеризацию.
может ты не понимаешь о чем мы с тобой беседуем?
или мб тебе стоило назвать тему точнее, например сложности выявления ранних стадий рака при профилактическом осмотре?
но ты посвятила тему диспансеризации и удивляешься почему я с тобой не соглашаюсь
да потому, что д-я это не только рак, но и туберкулез, например
и создавалась эта система тогда, когда никаких других методов массово обеспечить профилактику граждан не было
иди учи историю медицины, новаторша
или мб тебе стоило назвать тему точнее, например сложности выявления ранних стадий рака при профилактическом осмотре?
но ты посвятила тему диспансеризации и удивляешься почему я с тобой не соглашаюсь
да потому, что д-я это не только рак, но и туберкулез, например
и создавалась эта система тогда, когда никаких других методов массово обеспечить профилактику граждан не было
иди учи историю медицины, новаторша
Ты смыл слова профилактика вообще понимаешь? А смысл слова диспансеризация? Статью целиком прочитал? Рак - это только один из аспектов, в котором неэффективно, а их там множество, вообще-то.
в статье не только про рак, но и напрмер про болезни ссз =)
при том что делать экг весьма дёшево
а поголовная проверка на туберкулёз это жесть, не в колонии живём же
при том что делать экг весьма дёшево
а поголовная проверка на туберкулёз это жесть, не в колонии живём же
кстати, а ты понимаешь такую статистику как в статье? всмысле методов
Вот как раз проверка на туберкулёз - это хоть как-то эффективно, так как его уровень в РФ даже среди благополучного населения очень настораживающий.. В отличие от диспансеризации с целью профилактировать инфаркты или инсульты, к примеру.
Попробую объяснить на пальцах. Если существует
а)болезнь, у которой есть скрытый бессимптомный период течения
б) метод, который обладает достаточной чувствительностью в этом периоде болезни и который может иметь скрининговый формат
в) способ лечения или компенсации болезни либо общественная опасность болезни, при котрой больного надо выявить даже без наличия эффективного лечения
г) болезнь имеет достаточную распространённость в популяции
то при одновременном сочетании всех 4-х условий есть смысл организовать скрининг на эту болезнь.
С инфекциями, например, сифилисом или СПИДом, всё понятно
а) бессимптомный период есть
б) метод скринингового формата есть - анализы крови разного вида
в) общественная опасность и\или способы лечения есть
г) распространённость есть.
Со многими остальными патологиями обычно всё упирается в скрининговый достаточно чувствительный метод. У туберкулёза есть - это проба Манту (диаскин-тест) и флюорография. Из-за общественной опасности можно надавить на пациента в плане лечения, и то очень большая часть пациентов откровенно забивают на необходимость лечения, выращивая устойчивые формы. Т.е. низкая комплаентность населения,выращивание устойчивых форм в учреждениях ФСИН самим государством и добровольно населением социально низких страт делают диспансеризацию малоэффективной (её не проходят малообеспеченные социальные слои и заключённые, хотя именно им она нужна в первую очередь). Поэтому скрининговые исследования на туберкулёз стараются делать намного чаще, чем любые диспансеризации. Иначе это будет ещё менее эффективно.
С заболеваниями ССС намного сложнее. Гипертоническая болезнь вроде как в скрининговом формате обнаруживается- измерить АД, анализы на холестерин. А вот дальше по сути тупик - вылечиться от них нельзя - можно только контролировать всю жизнь препаратами и образом жизни, понять, у кого и когда будет инфаркт или инсульт по этим анализам тем более невозможно в принципе. Низкая комплаентность населения в этом вопросе сводит большинство усилий терапевтов в обнаружении гипертонической болезни на нет. Аналогичная ситуация с мерцательной аритмией - есть метод, есть препараты, но из-за невозможности вылечиться и низкой комплаентности эффект массового осмотра не отличается от эффекта добровольных одиночных посещений врача в масштабах населения. Но деньги тратятся на это очень большие. Не в коня корм, так сказать.
И если последовательно перебирать системы органов, то обнаружится на удивление мало состояний, которые вообще в принципе есть смысл массово скринировать. К таким, например, относится ХОБЛ - вот её есть смысл прицельно искать. Т.е. диспансеризация в виде - отправить к терапевту\хирургу\ окулисту\ итд, чтобы что-нить найти бессмысленно по определению. А вот если бы это мероприятие было прицельно в виде скринингов на КОНКРЕТНЫЕ диагнозы, исходя из пола, возраста и ещё чего-нить, причём диагнозы заведомо должны быть доказано эффективно скринируемыми, то вот тогда польза была бы. Сейчас же этого нет и не предвидится. Так как сама постановка вопроса в виде -наличия доказательств, что заболевание эффективно скринируемое в РФ отсутствует. Что многие пользователи флокала наглядно демонстрируют. Пример - скрининг на ПСА. Сейчас появляется всё больше исследований, что он настолько неспецифичен, что эффект от него близок к случайным вариациям.
Пример - возможно, я ошибаюсь, но полезен скрининг на ТТГ в большинстве регионов РФ, так как практически вся РФ - иододефицитный регион. Скрининг на диабет чрезвычайно полезен. Но тут низкая комплаентность пациентов его сведёт почти на нет, к сожалению.
Попробую объяснить на пальцах. Если существует
а)болезнь, у которой есть скрытый бессимптомный период течения
б) метод, который обладает достаточной чувствительностью в этом периоде болезни и который может иметь скрининговый формат
в) способ лечения или компенсации болезни либо общественная опасность болезни, при котрой больного надо выявить даже без наличия эффективного лечения
г) болезнь имеет достаточную распространённость в популяции
то при одновременном сочетании всех 4-х условий есть смысл организовать скрининг на эту болезнь.
С инфекциями, например, сифилисом или СПИДом, всё понятно
а) бессимптомный период есть
б) метод скринингового формата есть - анализы крови разного вида
в) общественная опасность и\или способы лечения есть
г) распространённость есть.
Со многими остальными патологиями обычно всё упирается в скрининговый достаточно чувствительный метод. У туберкулёза есть - это проба Манту (диаскин-тест) и флюорография. Из-за общественной опасности можно надавить на пациента в плане лечения, и то очень большая часть пациентов откровенно забивают на необходимость лечения, выращивая устойчивые формы. Т.е. низкая комплаентность населения,выращивание устойчивых форм в учреждениях ФСИН самим государством и добровольно населением социально низких страт делают диспансеризацию малоэффективной (её не проходят малообеспеченные социальные слои и заключённые, хотя именно им она нужна в первую очередь). Поэтому скрининговые исследования на туберкулёз стараются делать намного чаще, чем любые диспансеризации. Иначе это будет ещё менее эффективно.
С заболеваниями ССС намного сложнее. Гипертоническая болезнь вроде как в скрининговом формате обнаруживается- измерить АД, анализы на холестерин. А вот дальше по сути тупик - вылечиться от них нельзя - можно только контролировать всю жизнь препаратами и образом жизни, понять, у кого и когда будет инфаркт или инсульт по этим анализам тем более невозможно в принципе. Низкая комплаентность населения в этом вопросе сводит большинство усилий терапевтов в обнаружении гипертонической болезни на нет. Аналогичная ситуация с мерцательной аритмией - есть метод, есть препараты, но из-за невозможности вылечиться и низкой комплаентности эффект массового осмотра не отличается от эффекта добровольных одиночных посещений врача в масштабах населения. Но деньги тратятся на это очень большие. Не в коня корм, так сказать.
И если последовательно перебирать системы органов, то обнаружится на удивление мало состояний, которые вообще в принципе есть смысл массово скринировать. К таким, например, относится ХОБЛ - вот её есть смысл прицельно искать. Т.е. диспансеризация в виде - отправить к терапевту\хирургу\ окулисту\ итд, чтобы что-нить найти бессмысленно по определению. А вот если бы это мероприятие было прицельно в виде скринингов на КОНКРЕТНЫЕ диагнозы, исходя из пола, возраста и ещё чего-нить, причём диагнозы заведомо должны быть доказано эффективно скринируемыми, то вот тогда польза была бы. Сейчас же этого нет и не предвидится. Так как сама постановка вопроса в виде -наличия доказательств, что заболевание эффективно скринируемое в РФ отсутствует. Что многие пользователи флокала наглядно демонстрируют. Пример - скрининг на ПСА. Сейчас появляется всё больше исследований, что он настолько неспецифичен, что эффект от него близок к случайным вариациям.
Пример - возможно, я ошибаюсь, но полезен скрининг на ТТГ в большинстве регионов РФ, так как практически вся РФ - иододефицитный регион. Скрининг на диабет чрезвычайно полезен. Но тут низкая комплаентность пациентов его сведёт почти на нет, к сожалению.
И ещё кое-что отпишу. Большинство забывает о том, что у медицины может быть метод лечения или диагностики некоторой фигни. Но это не синоним того, что здравоохранение должно начать его использовать, и что использование будет эффективным в масштабах государства, к примеру. Именно поэтому эффект в разном масштабе тоже требует проверки. Так как гетерогенность популяции по всяческим параметрам может настолько варьировать отклик на лечение или диагностируемые параметры, что метод в массовом применении станет бессмысленным, так как неопределённость его результата будет перекрывать всю пользу даже для узко выделенной специфической группы. Эта вещь понятна естественникам, так как они сплошь и рядом видят её в эксперименте, но обычно очень плохо доходит до экономистов и других гуманитариев. Именно поэтому они запросто используют среднюю. В итоге средний вес муравья у них запросто достигает 700 кг. Или средняя температура по больнице - навязший в зубах пример, но не осознаваемый, похоже, тем же Пофигистом. Так как тот же туберкулёз начинать скринировать надо с учреждений ФСИН. И если там провал, то никакие скрининги благополучного населения не помогут в принципе, но зато позволят выкинуть деньги на ветер. Туберкулёз скринировать надо у обитателей социального дна, которые в жизни не пойдут ни на какую диспанеризацию. Это не значит, что благополучным не нужно делать флюрографию. Но у благополучных просто из-за более частого появления в больницах по любым поводам чаще выявляется туберкулёз относительно возможного его наличия даже без диспансеризаций. Т.е. диспансеризация как мероприятие по туберкулёзу не эффективна, хотя методы борьбы с ним есть. Но они не имеют отношения к формату диспансеризаций, и тем более не имеют отношения к формату, предложенному Минздраву.
Или средняя температура по больнице - навязший в зубах пример, но не осознаваемый, похоже, тем же Пофигистом. Так как тот же туберкулёз начинать скринировать надо с учреждений ФСИН. И если там провал, то никакие скрининги благополучного населения не помогут в принципе, но зато позволят выкинуть деньги на ветер. Туберкулёз скринировать надо у обитателей социального дна, которые в жизни не пойдут ни на какую диспанеризацию. Это не значит, что благополучным не нужно делать флюрографию. Но у благополучных просто из-за более частого появления в больницах по любым поводам чаще выявляется туберкулёз относительно возможного его наличия даже без диспансеризаций. Т.е. диспансеризация как мероприятие по туберкулёзу не эффективна, хотя методы борьбы с ним есть. Но они не имеют отношения к формату диспансеризаций, и тем более не имеют отношения к формату, предложенному Минздраву.проба манту это же фуфломецин
в том смысле что низкоспецифичная и часто ложнопозитивная и ложнонегативная
у меня до сих пор заметный шрам на плече с младенчества, еще в туберкулезный диспансер клали, имхо мне очень повезло не заразиться там в итоге
у меня до сих пор заметный шрам на плече с младенчества, еще в туберкулезный диспансер клали, имхо мне очень повезло не заразиться там в итоге
диспансеризация - это старые кости, нельзя ее, конечно, для выявления рака и ссз применять. Она нужна не в городах с высоким уровнем жизни, а в едренях и на зонах, где человек не может никак самостоятельно к врачу попасть. Про ограниченность ее по болезням выше по треду ты уже писала.
Сейчас диспансеризация может быть с успехом заменена мониторингом. Плюсов куча:
- гибкость и специфичность контроля: в зависимости от истории болезни, мониторятся нужны показатели (то, что диспансеризация способна выявить новые болезни, имхо, миф. Если нету в популяции туберкулеза, как-то странно его искать. А его наличие можно эпидемиологическим фоном определить
- дистанционность: глюкометры, тонометры, пульсометры, кардиографы население может уже сейчас приобретать, а через пару лет появятся норм сервисы по агрегации и управлению данными (с США уже есть, но только в корпоративном секторе ввиду особенностей их страховки
- экономичность: врачей не надо сгонять в одно место и пропускать миллионы населения через них, реакция идет адресно по отклонениям от _индивидуальных_ норм. Что еще лучше, обращения распределены во времени, не надо содержать огромную пропускную способность у инфраструктуры (ее, кстати, сейчас нет в России, я специально ходил по этой теме в поликлинику по место пост. реги, мне на простой анализ крови талон выдали на 10 дней вперед).
Диспансеризация в России живет как эхо централизованной структуры советского здравоохранения, которая уже порядком подразложилась, но только не в мозгах наших чиновников, которые упрямо игнорируют реальность: и экономическую, и технологическую.
Сейчас диспансеризация может быть с успехом заменена мониторингом. Плюсов куча:
- гибкость и специфичность контроля: в зависимости от истории болезни, мониторятся нужны показатели (то, что диспансеризация способна выявить новые болезни, имхо, миф. Если нету в популяции туберкулеза, как-то странно его искать. А его наличие можно эпидемиологическим фоном определить
- дистанционность: глюкометры, тонометры, пульсометры, кардиографы население может уже сейчас приобретать, а через пару лет появятся норм сервисы по агрегации и управлению данными (с США уже есть, но только в корпоративном секторе ввиду особенностей их страховки
- экономичность: врачей не надо сгонять в одно место и пропускать миллионы населения через них, реакция идет адресно по отклонениям от _индивидуальных_ норм. Что еще лучше, обращения распределены во времени, не надо содержать огромную пропускную способность у инфраструктуры (ее, кстати, сейчас нет в России, я специально ходил по этой теме в поликлинику по место пост. реги, мне на простой анализ крови талон выдали на 10 дней вперед).
Диспансеризация в России живет как эхо централизованной структуры советского здравоохранения, которая уже порядком подразложилась, но только не в мозгах наших чиновников, которые упрямо игнорируют реальность: и экономическую, и технологическую.
Ложнопозитивность Манту - да, есть, и прежде всего из-за перекрёстной реакции на БЦЖ. Но её масштабы преувеличены из-за безграмотности прививочных медсестёр - они часто меряют не папулу, а красноту. Диаскин тест даёт меньше ложнопозитивных реакций, и сейчас постепенно входит во фтизиатрическую практику РФ.
б) ложнонегативность прежде всего в ситуациях проблемы с иммунитетом пациента. Тут будут проблемы почти со всеми существующими тестами на туберкулёз, и Манту- не исключение. Квантифероновый, который чуть более чувствителен у иммунодефицитных пациентов, существует в РФ на птичьих правах, КТ имеет не скрининговый формат и далеко не прост в интерпретации. Ещё может быть ложнонегативным в случае нетипичной локализации туберкулёза. Но выявить его хоть чем-то - это вообще-то проблема, и повторюсь - Манту тут не исключение.
б) ложнонегативность прежде всего в ситуациях проблемы с иммунитетом пациента. Тут будут проблемы почти со всеми существующими тестами на туберкулёз, и Манту- не исключение. Квантифероновый, который чуть более чувствителен у иммунодефицитных пациентов, существует в РФ на птичьих правах, КТ имеет не скрининговый формат и далеко не прост в интерпретации. Ещё может быть ложнонегативным в случае нетипичной локализации туберкулёза. Но выявить его хоть чем-то - это вообще-то проблема, и повторюсь - Манту тут не исключение.
как думаешь следовало интерпретировать огромную гноящуюся язву глубиной до костей?
Понтия не имею - я не фтизиатр, и эту язву не вижу. Это было с БЦЖ или с Манту? Если от БЦЖ, то рубчик будет на наружной поверхности верней половины плечевой части руки, если от Манту - на внутренней поверхности нижней половины предплечья руки. Так где рубец-то?
Если с БЦЖ, то с некоторой вероятностью - БЦЖит. БЦЖит развивается по 2-м причинам.
а) Врождённая особенность иммунитета- сниженный иммунитет к Mycobacterium bovis. Есть у некоторого процента людей. Ликвидируется приёмом изониазида в течение нескольких месяцев. Могут заболеть туберкулёзом коров в отличие от остального населения.
б) Недоослабленная вакцина, т.е. привика была сделана плохо приготовленной вакциной. Ликвидируется тем же изониазидом. В дальнейшем никаких проблем не будет.
От криворукости делающих прививки может развиться холодный абсцесс.
Но вообще гноящаяся БЦЖ - это нормальный поствакцинальный процесс. Возможно, чуть более сильное нагноение, чем у других детей, и напугало родителей.
Если это было от пробы Манту,то первое, что я лично бы подумала - злостное нарушение правил асептики и антисептики. Второе - индивидуальная реакция. Но про такую индивидуальную реакцию на Манту я не слышала. Бывают фурункулы на АКДС - это да, особенности индивидуальной реакции. При этом они сами проходят обычно даже без вскрытия, что интересно.
В общем, бессмысленно гадать, что и как, не имея фотографий, выписок из истории болезни и т.д.на основании слов испуганных родителей. И тем более не будучи фтизиатрами. От БЦЖ у многих крупный рубчик на плече - его ещё путают с оспяным.
З.Ы. Увидела про плечо. Огромный-это какой? У моей мамы сантиметровый в диаметре шрам глубиной где-то 4-5 мм - последствия нормального поствакцинального процесса. Вот пример шрама на плече похожего происхождения (но ручаться не могу) http://pic.oscdn.net/pic/7946154/l
Но определить, что это было- БЦЖит из-за особенностей иммунитета\ недоослабленной вакцины или криворукость медперсонала или самостоятельный фурункул уже невозможно. Поэтому твои вопросы мне непонятны- подними свою детскую карточку и посмотри на диагноз. Или ты хочешь диагноза даже не по фото, а по "Рабинович напел"? Какая у тебя была Манту впоследствии по годам в мм, как нарастала по годам?
Если с БЦЖ, то с некоторой вероятностью - БЦЖит. БЦЖит развивается по 2-м причинам.
а) Врождённая особенность иммунитета- сниженный иммунитет к Mycobacterium bovis. Есть у некоторого процента людей. Ликвидируется приёмом изониазида в течение нескольких месяцев. Могут заболеть туберкулёзом коров в отличие от остального населения.
б) Недоослабленная вакцина, т.е. привика была сделана плохо приготовленной вакциной. Ликвидируется тем же изониазидом. В дальнейшем никаких проблем не будет.
От криворукости делающих прививки может развиться холодный абсцесс.
Но вообще гноящаяся БЦЖ - это нормальный поствакцинальный процесс. Возможно, чуть более сильное нагноение, чем у других детей, и напугало родителей.
Если это было от пробы Манту,то первое, что я лично бы подумала - злостное нарушение правил асептики и антисептики. Второе - индивидуальная реакция. Но про такую индивидуальную реакцию на Манту я не слышала. Бывают фурункулы на АКДС - это да, особенности индивидуальной реакции. При этом они сами проходят обычно даже без вскрытия, что интересно.
В общем, бессмысленно гадать, что и как, не имея фотографий, выписок из истории болезни и т.д.на основании слов испуганных родителей. И тем более не будучи фтизиатрами. От БЦЖ у многих крупный рубчик на плече - его ещё путают с оспяным.
З.Ы. Увидела про плечо. Огромный-это какой? У моей мамы сантиметровый в диаметре шрам глубиной где-то 4-5 мм - последствия нормального поствакцинального процесса.
Вот пример шрама на плече похожего происхождения (но ручаться не могу) http://pic.oscdn.net/pic/7946154/lНо определить, что это было- БЦЖит из-за особенностей иммунитета\ недоослабленной вакцины или криворукость медперсонала или самостоятельный фурункул уже невозможно. Поэтому твои вопросы мне непонятны- подними свою детскую карточку и посмотри на диагноз. Или ты хочешь диагноза даже не по фото, а по "Рабинович напел"? Какая у тебя была Манту впоследствии по годам в мм, как нарастала по годам?
с манту было 
карточка успешно протеряна, в какой-то их поликлиник забрали и не вернули
карточка успешно протеряна, в какой-то их поликлиник забрали и не вернули
С Манту на плече не может быть- только предплечье. Ты писала про шрам на плече.
тем не менее
туберкулезный диспансер точно не омжет быть связан с бцж
туберкулезный диспансер точно не омжет быть связан с бцж
туберкулезный диспансер точно не омжет быть связан с бцжЭто ты с чего решила?
Ладно, это всё оффтоп. Резюме - есть некая история о нагноении после укола, как-то связанного с туберкулёзом. Всё, что мне известно вообще и от тебя в частности, говорит мне, что это должен был быть БЦЖит. Причина уже покрыта мраком тайны.
Ты со мной не согласна и говоришь, что это из-за Манту, хотя ничего из того, что с Манту связано, за это объективно не говорит. За Манту говорят примерно те же факты, что и говорящие за аутизм от прививок, инсульты от прививок и т.д. на мамских форумах, что тобой же осуждаемо.
Я останусь при своём мнении и привычном мне способе рассуждений до появления новых фактов.
я это только со слов родителей знаю, какие новые факты?
более того, ни в коем раз не нуждаюсь в каких-либо деагнозах с форума
более того, ни в коем раз не нуждаюсь в каких-либо деагнозах с форума

valiya-liya
К вопросу о диспанеризации.http://www.nhshealthatwork.co.uk/images/library/files/Clinic...
Жду сторонников советских диспансеризаций.